A complex case of aortic coarctation with aortic arch aneurysm and arteriopathy of the aortic arch vessels: Comprehensive assessment with cardiovascular magnetic resonance imaging
Alexios S. Antonopoulos1, Eva Nyktari1, Raad H Mohiaddin1,2
1CMR Unit Royal Brompton Hospital, London UK
2National Heart and Lung Institute, Imperial College London
Clinical Presentation:
A 38-year-old female with a history of complicated aortic coarctation with multiple vascular abnormalities underwent cardiovascular magnetic resonance (CMR) and contrast-enhanced magnetic resonance angiography (CE-MRA) imaging to assess the aorta and neck vessel anatomy to guide surgical repair.
CMR Findings: A contrast enhanced-magnetic resonance angiography (CE-MRA) of the aorta showed a normal size ascending aorta and a mildly hypoplastic arch (16mm) with upward angling (gothic appearance) tapering down to 12mm before forming a true lobulated aneurysmal segment (39x40x35mm), which extended for ~60mm from mid arch to the proximal descending thoracic aorta. No mural or intracavity thrombus was identified (Figure 1 & 2 and Video 1). The distal neck of the aneurysm measured ~ 11mm and the descending aorta was 21mm. Peak recorded velocity was 1.5m/s at the proximal aneurysm neck and 1.6m/s near the distal neck, with no significant diastolic tail (suggesting that the aortic coarctation was not hemodynamically significant). The right innominate artery (12mm at origin) bifurcated into the right common carotid and a tortuous right subclavian (both 7-8mm at origin), the latter giving rise to the right vertebral artery (~3mm) as normal. An atretic, tortuous (2-3mm) left common carotid artery arise superiorly from the hypoplastic arch ~10mm proximal to the origin of the aneurysmal segment.
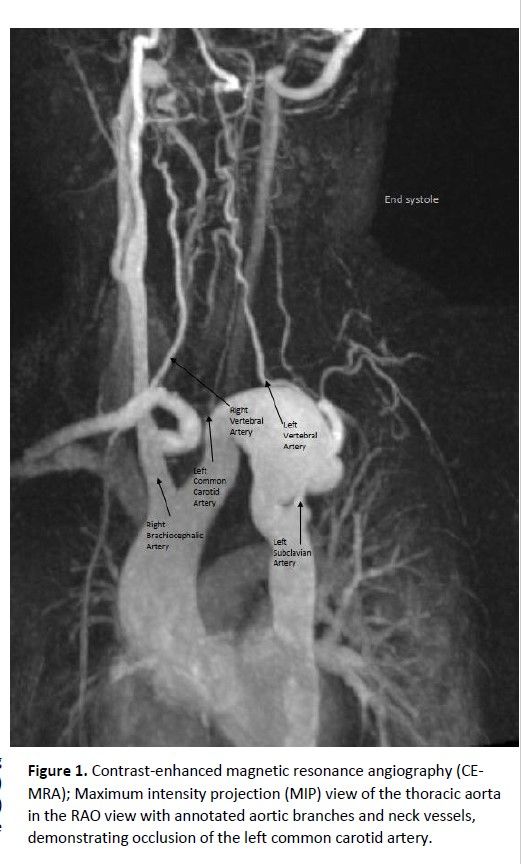
Video 1: Balanced steady-state free precession (bSSFP) imaging by cardiovascular magnetic resonance showing flow acceleration at the coarctation site and at the distal nek of the aortic aneurysm
The left subclavian (~6mm) arise posteriorly from the descending aorta just distal to the aneurysm
and run a posterior course to the aneurysm before supplying the left vertebral artery. Flow was
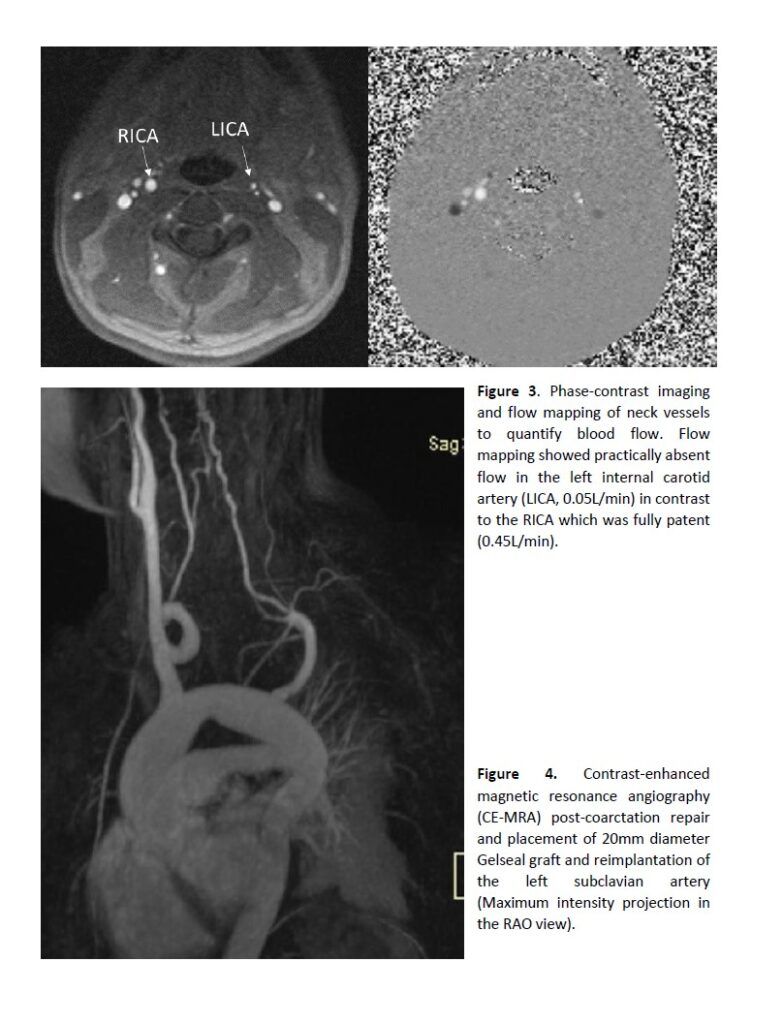
antegrade in both common carotid and vertebral arteries. CMR phase contrast flow measurement in
the main branches were as follow: Right brachiocephalic artery: 1.44L/min, Right internal carotid
artery: 0.45L/min, Left internal carotid artery: 0.05L/min, Left subclavian artery: 0.30L/min (Figure 3).
Based on these useful anatomical details the patient was referred for surgery. Aortic arch aneurysm
was excised with placement of a 20mm diameter Gelseal interposition graft and re-implantation of
the left subclavian artery (figure 4).
Discussion
Coarctation of the aorta is a pathological narrowing of the aortic arch which can be discrete or diffuse.
The coarctation site typically involves the aortic segment at the site of arterial duct (juxta ductal) but
occasionally may affect other segments too. According to the latest guidelines for the management of
patients with adult congenital heart disease, every adult with coarctation (repaired or not) should
have at least one cardiovascular MRI or CT scan for complete evaluation of the thoracic aorta and
intracranial vessels.1 Whilst echocardiography may be used to assess aortic arch morphology and
pressure gradients at the coarctation site, CMR imaging offers specific advantages over
echocardiography. CMR allows the anatomic description of coarctation and the assessment of aortic
arch anatomy and neck vessel branching pattern. The hemodynamic significance of the coarctation
can also be assessed by the presence of diastolic flow tail at the coarctation site, the presence of
arterial collaterals and the quantification of collateral aortic flow (by phase contrast flow mapping in ascending aorta, prior to coarctation, post coarctation and at the diaphragm). CMR-derived hemodynamic and anatomic data can help determine the hemodynamic significance of coarctation2. In addition, CMR provides diagnostic information on left ventricle volumes/hypertrophy and aortic valve function at the same time. In the present rare and complex case of aortic coarctation with associated aortic aneurysm and neck vessels’ arteriopathy, the anatomical and blood flow information provided by CMR was crucial to the surgical planning and management. CMR herein provided detailed anatomical information on aortic arch anatomy, aneurysm size and exact location and the branching pattern of neck vessels in relation to the aortic aneurysm site. Furthermore, blood flow information was crucial for detecting the occlusion of the left internal carotid artery in this case. Compared to computed tomography angiography (CTA), CMR offers the advantage of no ionizing radiation use and functional/hemodynamic information, which CTA cannot provide. For this reason, CMR has the primary role as the modality of choice for the long-term screening of these patients before coarctation repair for the progression of coarctation as well as after surgical correction of the coarctation for complications, re-coarctation, and aneurysm development.3
Key Learning Points
• Cardiovascular magnetic resonance (CMR) is the imaging modality of choice for the long-term screening of patients before and after coarctation repair.
• CMR offers excellent anatomical information on aortic arch anatomy and neck vessel status and branching pattern.
• CMR also provides functional information on the hemodynamic significance of the coarctation, the presence of arterial collaterals and quantification of collateral aortic flow
References
1. Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, Lung B, Kluin J, Lang IM, Meijboom F, Moons P, Mulder BJM, Oechslin E, Roos-Hesselink JW, Schwerzmann M, Sondergaard L, Zeppenfeld K and Group ESCSD. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2020.
2. Nielsen JC, Powell AJ, Gauvreau K, Marcus EN, Prakash A and Geva T. Magnetic resonance imaging predictors of coarctation severity. Circulation. 2005;111:622-8.
3. Chen SS, Dimopoulos K, Alonso-Gonzalez R, Liodakis E, Teijeira-Fernandez E, Alvarez-Barredo M, Kempny A, Diller G, Uebing A, Shore D, Swan L, Kilner PJ, Gatzoulis MA and Mohiaddin RH. Prevalence and prognostic implication of restenosis or dilatation at the aortic coarctation repair site assessed by cardiovascular MRI in adult patients late after coarctation repair. Int J Cardiol. 2014;173:209-15.
Legends to